

The Secret Solution to Sky Rocketing Drug Prices
Are you ready for this?


Over the last decade, the actual cost to produce most generic medications dropped substantially. Despite production cost reductions, retail sticker prices and patient co-pays continue to rise dramatically. Huh? Riddle me that.
Why is this happening? And what is the solution? To understand how decreasing production costs result in increasing retail prices-a phenomenon that seems to defy basic economic principals-it’s important to understand the role of Pharmacy Benefit Managers (PBMs).
Pharmacy Benefit Managers first arose in the late 1960’s. With increasing medication options and insurance market consolidation, PBMs promised to act as intermediaries between insurance companies, pharmaceutical companies, and pharmacies to lower the cost of prescription medications for payors and patients. Currently, the three largest PBM players- CVS Caremark, Express Scripts, and OptumRx- control almost 80% of insured Americans’ drug prices. That’s some serious industry dominance.
The PBM promise was appealing. But it didn’t pan out as advertised. A growing body of research suggests that PBMs profit by artificially inflating drug prices, capturing portions of the discounts they negotiate for insurers, and pocketing the difference. Essentially, PBMs negotiate a lower medication price directly with the manufacturer, then charge independent pharmacies and insurance plans a substantially higher price and pocket the difference as profits. When there are two versions of the same or similar medications, they often make exclusivity deals with the pricier version. This results in the more expensive version being added to the insurance formulary. Then they pocket the difference in costs to themselves as profits, which they rename “rebates.” To be clear, the price increase gets passed on to you- the consumer-and the struggling independent pharmacies.
For a much deeper dive into the actual mechanics of this well-shrouded process, I encourage you to check out last month’s New York Times exposé on PBMs entitled The Opaque Industry Secretly Inflating Prices for Prescription Drugs. Following these publications, last Tuesday The Federal Trade Commission released a scathing 71-page report sharply rebuking PBMs and saying, “These powerful middlemen may be profiting by inflating drug costs and squeezing Main Street pharmacies.”
PBM overinfluence abounds. And the decisions are always profit-driven, often at the expense of patient safety. Here are just two everyday examples:
1. Mandatory 90-day fills
Express Scripts, which operates predominantly as a mail order pharmacy, now requires prescribers to submit most prescriptions as a 90-day supply, versus smaller but more frequent amounts. Express Scripts saves on shipping costs. This is a sound financial decision, but a very problematic clinical decision. When starting a medication, it’s challenging to predict the optimal dose. It often takes small, frequent dose increases to reach the most clinically effective dose-something that is at odds with the Express Script 90-day preference. Additionally, Psychiatrists often work with patients who struggle with self-harm thoughts. These patients are at an increased risk of self-harm/suicide attempts. In these scenarios, it’s not safe to prescribe larger amounts of medications that could be potentially lethal in an overdose.
2. More expensive medication versions on Medicare/Medicaid/HMO formularies
Buprenorphine/Naloxone, otherwise known as Suboxone, is a life-saving medication used to treat Opioid Use Disorder. It comes in a film version and a tablet version. Both have the exact same active ingredients. The Suboxone film manufacturer price is about twenty times more expensive than the Suboxone tablet price. However, the much pricier Suboxone film is the only approved version on many state Medicaid formularies. At the risk of stating the obvious, this makes zero financial sense. Why pay for the Lamborghini when the Kia will also get us there? PBMs choose the Lamborghini over the Kia and pass the price hike on to you-while pocketing the “rebates” (profits) and kickbacks. In the case of Medicare and Medicaid, the price hikes are passed on to all of us: the American taxpayers.
Clearly PBMs need more comprehensive and objective regulatory oversight. The FTC and Congress seem to be listening. Last year, Congress launched a formal, ongoing investigation into PBMs’ role in rising healthcare costs. The FTC report followed last month.
But the rusty wheels of federal regulation reform move slow. Very slow. There might be a more immediate and ultimately more powerful positive disrupter to the PBM drug pricing dominance: enter Mark Cuban’s Cost-Plus Pharmacy.
Being equally disenchanted with PBM middleman medication mark-ups, Radiologist Alexander Oshmyansky and businessman Mark Cuban launched Cost-Plus Pharmacy in January 2022 with the goal of removing PBM middlemen entirely and thus lowering drug costs. Cost-Plus Pharmacy purchases medications directly from the manufacturer, with no middleman mark-up. Cost-Plus Pharmacy contracts directly with generic pharmaceutical manufacturers. Then they use accredited pharmacists to fill and mail prescriptions directly to the patient.
Cost-Plus Pharmacy uses a refreshingly transparent fixed pricing strategy. The final cost to the consumer is simply the manufacturer cost “plus” a fixed percentage. Often utilized in military contract bids, cost-plus pricing is a method that utilizes an open, transparent, fixed percentage markup price. The cost clarity increases consumer buying confidence and competition. For Cost-Plus Pharmacy, the patient only pays the original medication manufacturer production cost, plus a 15% markup to cover operational costs, with a $5 pharmacy filling fee, and a $5 shipping cost. No need for insurance or PBMs. The resulting lower prices are truly staggering.
As of June 2022, Cost-Plus Pharmacy had approximately 100 medications available. In late 2023, that number grew to over 2,200 available medications. Check out their complete list here. The large selection and low costs are game changers to both uninsured and insured patients alike. In many cases, the Cost-Plus Pharmacy price is cheaper than even an insured patient’s final price would be at a local pharmacy. Plus, you get the added convenience of shipping right to your doorstep. For example, the retail price of Lexapro, a common prescription medication used for depression and anxiety, can run anywhere from $50-$150. The average out- of-pocket cost for an insured patient is $20. The Cost-Plus Pharmacy price for a 30-day supply is $6.50. Wowza!
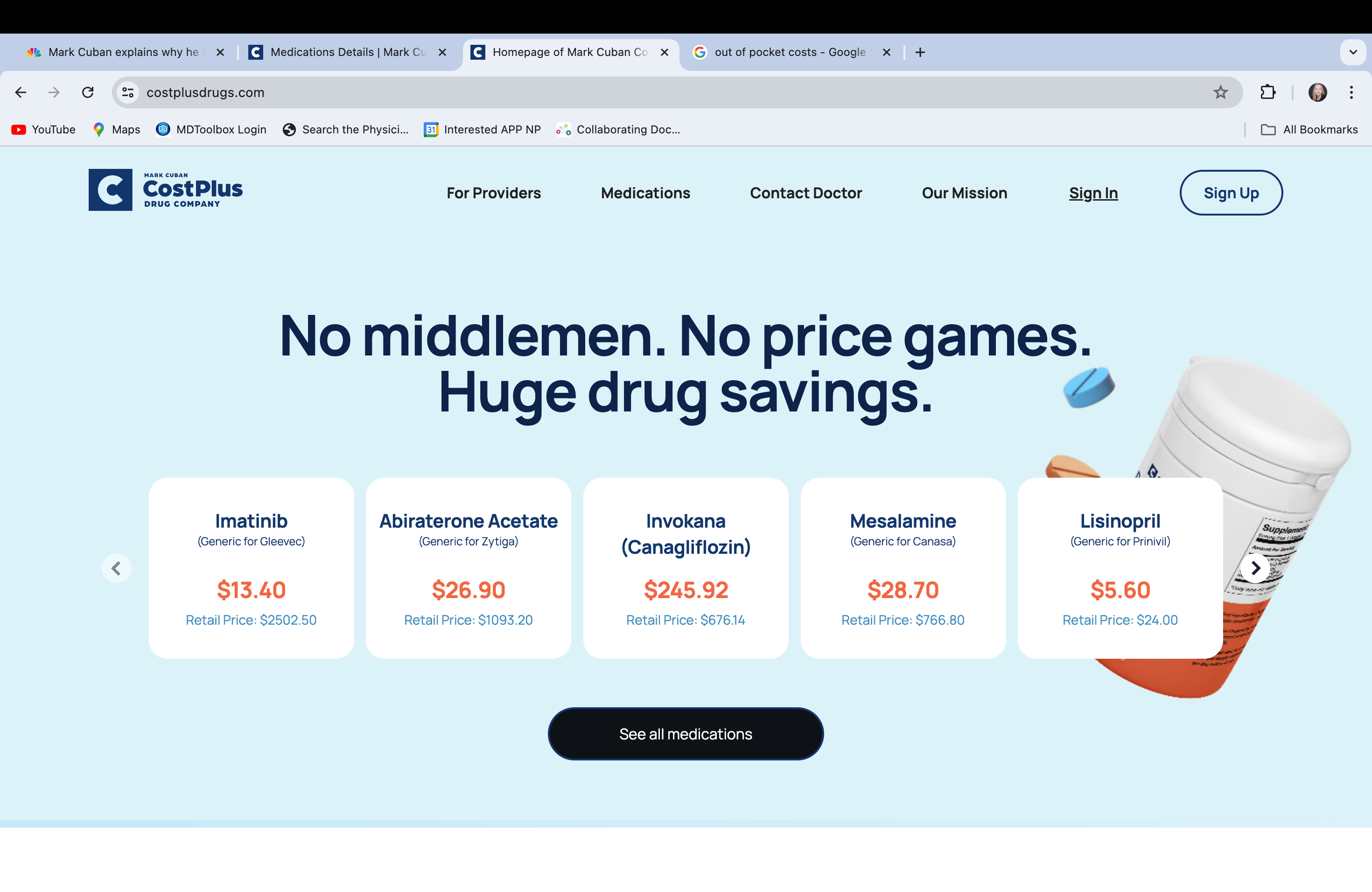
Cost-Plus Pharmacy Homepage
Patients and providers can sign up for Cost-Plus Pharmacy services through their user-friendly website. The provider electronically sends the prescription directly to Cost-Plus Pharmacy for filling and shipping. Cost-Plus Pharmacy ships to all 50 states.
Mark Cuban recently sold his majority stake in the Dallas Mavericks. He used the proceeds to build a 22,000-square-foot factory in Deep Ellum, Dallas for the purpose of manufacturing drugs completely in-house for Cost-Plus Pharmacy.
It worries me that even with a 15% mark-up and $10 pharmacy/shipping fee, the Cost-Plus Pharmacy medication prices are much lower than the price of medication through traditional insurance. Where is the difference going? I’m looking in the direction of the PBMs. PBM mark-ups also get passed on to smaller independent pharmacies, resulting in a financial strain that makes it challenging for most non-chain pharmacies to stay in business.
The growing awareness and utilization of Cost-Plus Pharmacy offers us a path to circumvent middleman markups in the American pharmaceutical market. For the very first time, it offers a better alternative. More use of Cost-Plus Pharmacy will result in less reliance on traditional PBM up charged pathways. As a growing, more affordable competitor, Cost-Plus Pharmacy could force PBMs to adjust their obtuse pricing strategies quicker than any regulator in Washington DC.
I applaud the FTC and Congress for increased PBM scrutiny and more regulatory oversight. But can we also take advantage of market dynamics and a strong competitor to force PBMs to evolve faster? I hope so. Nobody thought Blockbuster would ever go out of business. Until Netflix arrived. Nobody could imagine Blackberries would vanish. Until the arrival of the iPhone. Nobody could envision Kodak filing for bankruptcy. Until digital cameras came to the scene. This could be our Netflix of the pharmacy world.
In a profit driven society where cash is king, fierce competition with a superior product will be the biggest threat to PBM dominance-and our best hope for change.
-Lauren

Lauren, this is super interesting, I had not been fully aware of PBMs and their role in the drive up of costs. When I have worked with patients in free clinics who tried to get standard generic medications filled and came back to me quoting sky high prices, this all makes sense now. Thank you for highlighting this.